
Many traumatic injuries result in outwardly gruesome and visually grotesque injuries. Abdominal trauma however, often can go unnoticed and can be a silent killer if the injuries go unrecognized or untreated. While skeletal injuries often present with obvious deformity and are easily recognized, abdominal injuries are much more difficult to identify. In regards to traumatic injuries and death, blunt trauma to the abdomen leads all other forms of traumatic injury in morbidity and mortality. The abdominal cavity contains organs of the reproductive, gastrointestinal, genitourinary, endocrine and renal systems just to name a few. Many of these organs are extremely vascular and can lead to life threatening exsanguination of they are injured due to either blunt or penetrating trauma. Early recognition and a high index of suspicion for hemodynamic deterioration can often prevent or limit downstream complications both within and outside of the cavity itself.
The abdominal cavity is the largest cavity in the body. It is bordered by the diaphragm superiorly and the pelvis inferiorly. Often it is almost impossible to accurately decipher exactly which organ is injured and to what extent due to abdominal trauma, but rapid identification and aggressive treatment with transport to an appropriate facility can make the difference between life and death. Most abdominal organs are not afforded a large amount of protection from the musculoskeletal system like the thoracic cavity is so injuries can range from minor to life threatening. Often more than one organ system is injured and therefore the odds of life altering complications can often accompany any traumatic insult involving the abdomen itself.
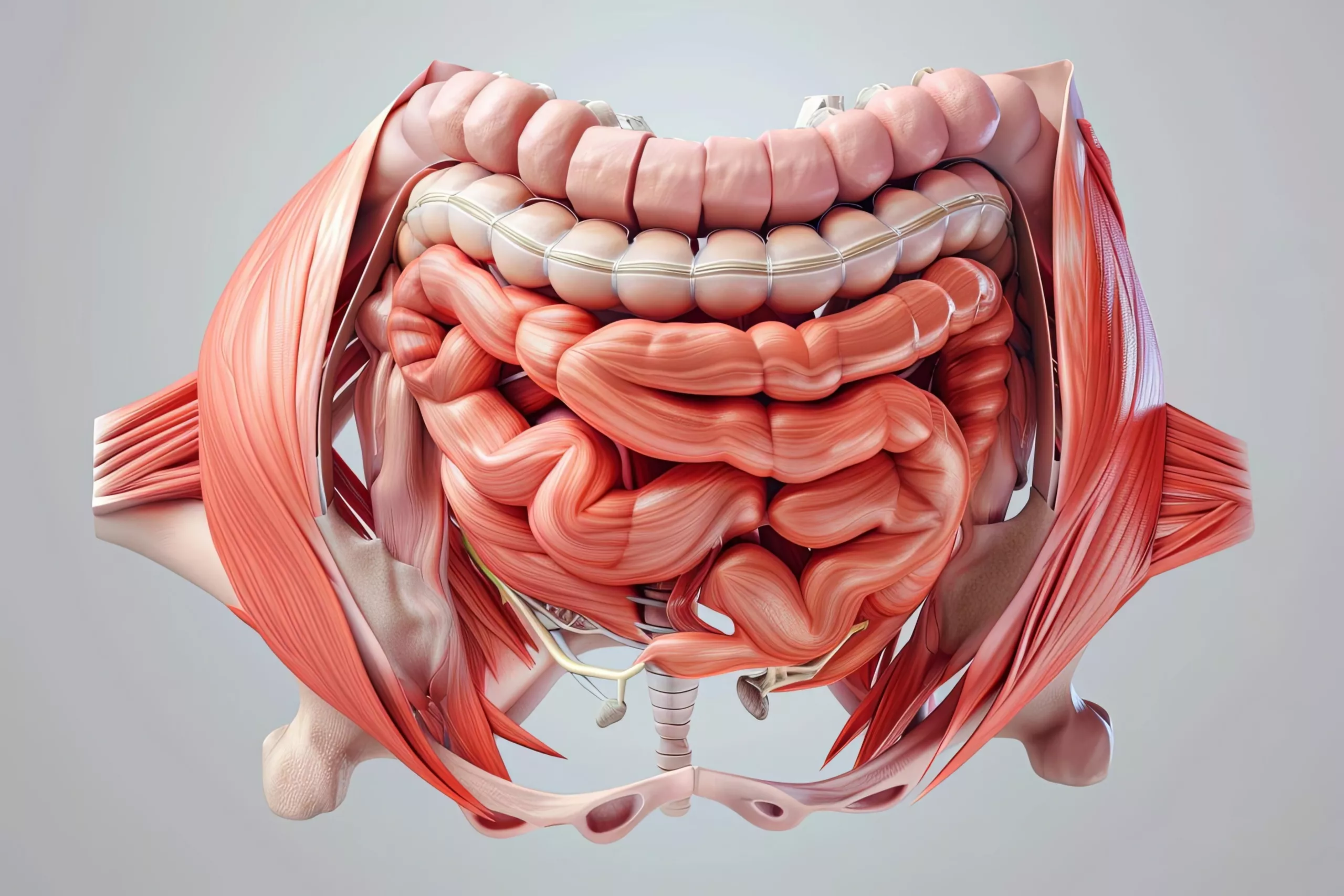
Scientific 3D illustration of abdominal muscles depicting hernias, with a clinical color mood
The liver and the spleen are the most frequently injured abdominal organs accounting for approximately 25% of all solid abdominal organ injuries. The liver, located in the right upper quadrant of the abdomen weighs around 3 pounds and is the most frequently injured solid organ of the abdomen. The liver is responsible for filtering incoming blood from the digestive tract, metabolizing drugs, detoxifying chemicals, secreting bile and making proteins that enhance clotting. Humans cannot live without their liver but they can live with a partial liver and it can actually grow back within a matter of months. The spleen is located in the left upper quadrant and is the second most frequently injured abdominal solid organ. The spleen stores around 1/3 of the the body’s platelets and also stores mature T and B lymphocytes. Old red blood cells are also cleared from the body via the spleen. Often when solid organs are damaged due to trauma, they will bleed. Bleeding into the abdominal cavity from solid organ injury can result in pain as the blood will often irritate the thin layer that lines the abdominal cavity and its organs, this is known as the peritonitis.
Hollow organs such as the stomach, urinary bladder, esophagus and small and large intestines will often spill their contents when injured during trauma. While bleeding is not as much of a concern as it is with solid organ abdominal injury, life threatening infection can occur and the patient can rapidly and irreversibly become septic. The spilling of urine, feces or partially digested food into the abdominal cavity can lead to severe, life threatening consequences. The same peritonitis that is caused by bleeding into the abdominal cavity can be caused by the spilling and ensuing irritation and infection of the abdominal cavity.
A thorough patient assessment and early, aggressive intervention can markedly improve outcomes in patients suffering from abdominal trauma whether it is due to blunt or penetrating injury. Recognition of the early signs and symptoms of shock can often prevent further vital sign deterioration. Waiting until the abdominal injury becomes openly evident can have catastrophic effects due the fact that abdominal trauma is frequently insidious and will progress rapidly. By the time the patient becomes symptomatic, the downward spiral has already progressed to the point of long term disability and/ or death. Rapid transport to a facility that can aggressively and adequately treat the abdominal trauma is an important part to damage control resuscitation. Performing interventions enroute instead of on the scene and pro actively treating the patient for shock will have a marked effect on morbidity and mortality. While advanced life support interventions such as IV fluid replacement and blood product infusion can make a difference, early, thorough assessment with a high index of suspicion and treating shock pro actively has shown to have a greater effect on minimizing death and disability in the abdominal trauma patient.