Many EMS providers have difficulty deciphering the difference between Placenta Previa and Abruptio Placenta in the field. While both conditions have some signs and symptoms as well as risk factors in common, each has its own defining factors and presenting symptomology such as the presence and consistency of vaginal bleeding. In this article we will outline both in regards to risk factors, patient presentation, pathophysiology and treatment modalities.
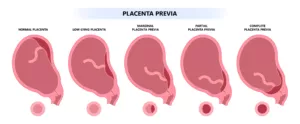
Placenta Previa occurs in roughly 1 out of every 200 pregnancies and is the most common cause of post delivery bleeding. It occurs when the placenta begins to expand over the outlet of the uterus and most often occurs in the second and/or third trimester. Asian women are much more likely to experience Placenta Previa over white women. Risk factors include previous cesarean sections, smoking, alcohol and/or cocaine use as well as a prior history of pregnancies complicated by Placenta Previa. It most often is diagnosed after the 20th week gestation via ultrasound examination. A low lying placental/uterine insertion location is most often the earliest sign of a potential Placenta Previa later in the pregnancy. As the placenta increases in size during the gestational period, the placental can partially or completely cover the inferior uterine outlet that leads to the “birth canal”. It is important to note, however that not all low lying placental insertions will result in Placenta Previa. More often than not a low lying placental insertion will actually “migrate or grow” up towards the fundus rather than migrating downward towards the cervix due to the larger amount of uterine wall blood flow present in the superior uterine regions. Most women who suffer from Placenta Previa will report the presence of painless bright red bleeding with a non tender, non rigid abdomen and the amount of bleeding will vary based on the percentage of placental growth over the uterine outlet. Abruptio Placenta is about twice as common as Placenta Previa at a frequency rate of around 1 per 100 pregnancies.
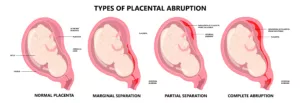
Abruptio Placenta occurs when a portion or the entire placenta is peeled away from the uterine wall. 80% of women that present with Abruptio Placenta will present with a painful, rigid abdomen and dark red vaginal bleeding. The presence or absence of vaginal bleeding depends on whether or not the accumulated blood gets trapped within the separated portion. Risk factors for Abruptio Placenta include the presence of fetal twins, smoking, African American ethnicity, chronic untreated hypertension, infectious processes, abdominal trauma during pregnancy, diabetes and heart disease. Abruptions can be either chronic or acute as it pertains to onset and can vary in presenting symptoms. Mild cases are often not recognized without an ultrasound and are often treated with bed rest, exercise and sexual activity limitations and frequent monitoring during the pregnancy. More severe cases that involve a larger portion of the placenta being dislodged from the uterine wall can present with hypovolemic shock, consistent prolonged uterine contractions due to the accumulating blood irritating the wall of the uterus and a tender rigid abdomen accompanied by bright red bleeding. In severe cases, the baby is often delivered via an emergent c-section as the fetal mortality rate can reach 80% and maternal mortality rate.
In the field, treatment will often involve assessment and maintenance of the ABC’s, having a high index of suspicion for potential vital sign deterioration, monitoring of fetal heart rate, aggressive pro active fluid resuscitation if necessary if the patient is hypotensive and transport to an appropriate facility capable of handling the issue at hand. Most complications of pregnancy are often diagnosed early due to technological advances and pro active pre natal care, but some of the patients slip through the cracks and may require EMS intervention. Keep in mind that these patients are often physiologically unique due to pregnancy related body changes and are at risk for rapid deterioration and should be treated with a high index of suspicion for deterioration.